
• Pain and inflammation may accompany infection and are sometimes manifested
by swelling, erythema, tenderness, and purulent drainage. Unfortunately,
these signs may be apparent only if the infection is superficial or in a
bone or joint.
• The manifestations of inflammation with deep-seated infections such as
meningitis, pneumonia, endocarditis, and urinary tract infection must be
ascertained by examining tissues or fluids. For example, the presence of
polymorphonuclear leukocytes (neutrophils) in spinal fluid, lung secretions
(sputum), and urine is highly suggestive of bacterial infection.
IDENTIFICATION OF THE PATHOGEN
• Infected body materials must be sampled, if at all possible or practical,
before the institution of antimicrobial therapy, for two reasons. First, a
Gram stain of the material may reveal bacteria, or an acid-fast stain may
detect mycobacteria or actinomycetes. Second, a delay in obtaining
infected fluids or tissues until after therapy is started may result in falsenegative
culture results or alterations in the cellular and chemical composition
of infected fluids.
• Blood cultures should be performed in the acutely ill, febrile patient. Less
accessible fluids or tissues are obtained when needed to assess localized
signs or symptoms (e.g., spinal fluid in meningitis, joint fluid in arthritis).
Abscesses and cellulitic areas should also be aspirated.
• Caution must be used in the evaluation of positive culture results from
normally sterile sites (e.g., blood, cerebrospinal fluid, joint fluid). The
recovery of bacteria normally found on the skin in large quantities (e.g.,
coagulase-negative staphylococci, diphtheroids) from one of these sites
may be a result of contamination of the specimen rather than a true
infection.
SELECTION OF PRESUMPTIVE THERAPY
• To select rational antimicrobial therapy for a given infection, a variety of
factors must be considered, including the severity and acuity of the disease,
host factors, factors related to the drugs used, and the necessity for use of
multiple agents.
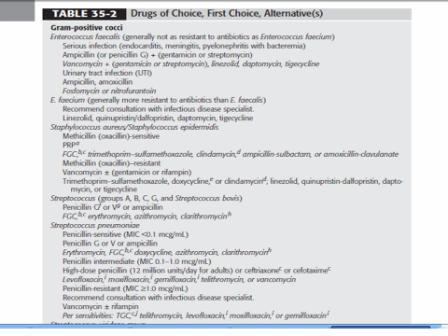
• There are generally accepted drugs of choice for the treatment of most
pathogens (Table 35-2). The drugs of choice are compiled from a variety
of sources and are intended as guidelines rather than specific rules for
antimicrobial use.
• When selecting antimicrobial regimens, local susceptibility data should be
considered whenever possible rather than information published by other
institutions or national compilations.
HOST FACTORS
• When evaluating a patient for initial or empiric therapy, the following
factors should be considered:
✓ Allergy or history of adverse drug reactions
✓ Age of patient
✓ Pregnancy
✓ Metabolic abnormalities
✓ Renal and hepatic function
✓ Concomitant drug therapy
• Concomitant disease states. A list of selected drug interactions involving
antimicrobials is provided in Table 35-3.
• Patients with diminished renal and/or hepatic function will accumulate
certain drugs unless dosage is adjusted. Any concomitant therapy the
patient is receiving may influence the selection of drug therapy, the dose,
and monitoring.
DRUG FACTORS
• Integration of both pharmacokinetic and pharmacodynamic properties of
an agent is important when choosing antimicrobial therapy to ensure
efficacy and prevent resistance. Antibiotics may demonstrate concentration-
dependent (aminoglycosides and fluoroquinolones) or time-dependent
(
β-lactams) bactericidal effects.
• The importance of tissue penetration varies with the site of infection. The
CNS is one body site where the importance of antimicrobial penetration is
relatively well defined and correlations with clinical outcomes are established.
Drugs that do not reach significant concentrations in cerebrospinal
fluid should either be avoided or instilled directly when treating meningitis.
• Apart from the bloodstream, other body fluids where drug concentration
data are clinically relevant include urine, synovial fluid, and peritoneal fluid.
• Pharmacokinetic parameters such as area under the concentration-time
curve (AUC) and maximal plasma concentration can be predictive of
treatment outcome when specific ratios of AUC or maximal plasma concentration
to the minimum inhibitory concentration (MIC) are achieved. For some agents, the ratio of AUC to MIC, peak-to-MIC ratio, or the time that
the drug concentration is above the MIC may predict efficacy.
• The most important pharmacodynamic relationship for antimicrobials
that display time-dependent bactericidal effects is the duration that drug
concentrations exceed the MIC.
No comments:
Post a Comment